Stress in crisis managers: evidence from self-report and psychophysiological assessments
Version 1 Released on 25 May 2016 under Creative Commons Attribution 4.0 International LicenseAuthors' affiliations
- Institute of Psychology, Department of Psychology and Medical Sciences - University for Health Sciences, Medical Informatics and Technology (UMIT)
- Department Psychologie, Fakultät für Psychologie und Pädagogik - Ludwig-Maximilians-Universität München
- Departamento de Personalidad, Evaluación y Tratamiento Psicológico - Universidad de Granada *. Unregistered author (unverified)
Keywords
- Psychological measurement
- Psychology
- Stress
Abstract
Directing disaster operations represents a major professional challenge. Despite its importance to health and professional performance, research on stress in crisis management remains scarce. The present study aimed to investigate self-reported stress and psychophysiological stress responses in crisis managers. For this purpose, 30 crisis managers were compared with 30 managers from other disciplines, in terms of self-reported stress, health status and psychophysiological reactivity to crisis-related and non-specific visual and acoustic aversive stimuli and cognitive challenge. Crisis managers reported lower stress levels, a more positive strain-recuperation-balance, greater social resources, reduced physical symptoms, as well as more physical exercise and less alcohol consumption. They exhibited diminished electrodermal and heart rate respon- ses to crisis-related and non-specific stressors. The results indicate reduced stress and physical complaints, dimin- ished psychophysiological stress reactivity, and a healthier life-style in crisis managers. Improved stress resistance may limit vulnerability to stress-related performance decline and facilitate preparedness for major incidents.
Introduction
Major incidents are characterized as sudden events, affecting large numbers of people, which overwhelm local health care and infrastructure and have a serious immediate and long-term impact on human welfare, public health and the environment. Major incidents encompass natural catastrophes such as floods, earthquakes and forest fires, in addition to human-made disasters including terror attacks or railway accidents, and industrial incidents like chemical spills or nuclear accidents. Some evidence confirms a global increase in the frequency and severity of major incidents in recent years (e.g., [27,45]); the importance of adequate preparedness is paramount, with a number of guidelines developed aiming to optimize crisis management, to provide adequate medical and social support to victims and to limit deleterious public health consequences (e.g., [56,54,16]).
Working in crisis environments represents a major challenge for professionals such as emergency workers, firefighters and medical or paramedical staff ([1]). This particularly applies to executive personal engaged in directing disaster operations, i.e. crisis managers; their duties include the mobilization and coordination of first responders, allocation of tasks, communication with authorities, evaluation of immediate needs of the affected population and ongoing risk assessment in order to maintain the security of victims and emergency personal. Crisis management involves high-level decision-making and principal responsibility for personnel, thereby requiring distinct organizational and leadership skills. The present study is concerned with self-reported stress and psychophysiological stress responses in crisis managers. While previous stress research almost exclusively focused on victims of disasters and first responders (e.g., [5,31,17]) , research on executive personnel remains scarce. Similarly to first responders, during operations crisis managers are exposed to severe suffering, injury and death, which in many cases can be regarded as traumatic stressors (e.g., [6]). Holding a leadership position also necessitates further challenges; in addition to great responsibility for personnel and human lives, crisis managers may also be faced with conflicts of interest, insufficient manpower, ambiguous or conflicting roles and extremely high expectations from others. The stress burden is considerably lower during normal working activities between actual disaster relief operations, in which managers perform executive functions involving administrational and personnel management. These tasks are frequently associated with occupational or organisational stressors such as conflict with authorities and co-workers, time-consuming administrative duties, overwork or work-life conflicts (e.g., [4]). Institutions responsible for disaster management typically comprise various units, pertaining for example to civil protection and fire and rescue services, and are characterized by complex organisational and hierarchical structures. Thus, in terms of size and complexity disaster management organisations may be comparable to companies situated within the fields of economy and industry.
The impact of sustained stress on mental and physical health is very well-documented (e.g., [13]). Several studies indicate reduced emotional wellbeing and increased self-reported stress, posttraumatic symptoms, depression and alcohol abuse in emergency medical personnel and firefighters [1,5,31,24]. However, it appears that only a subgroup of rescue workers are affected; moreover, various predictors have been identified that modify symptom occurrence. High levels of social support are associated with reduced posttraumatic and additional psychic symptoms [51,63], while active task-oriented coping-styles are connected with lower emotional and bodily stress [14,38]. Further factors reducing distress include job satisfaction and internal locus of control, as well as sufficient recovery time between operations [1,14].
The specific professional conditions encountered by crisis managers may contribute to the development of coping-skills and psychophysiological stress-resistance, in the context of which flexibility may play an important role. Psychological flexibility refers to an individual's ability to efficiently adapt to changing situational demands, to adjust mental and behavioral resources to suit current requirements and to cope with negative emotions and burdensome experiences [33,55]. While inflexibility has been implicated in various psychopathological conditions, a high degree of flexibility may mitigate against the deleterious effects of stress, thereby promoting health and wellbeing [9,55,33]. The working conditions of crisis managers involve rapid switching between regular management duties and extremely demanding disaster relief operations, which requires sudden activation of mental and physical resources followed by a quick return to the initial state. It could be hypothesized that these challenges may improve crisis managers' ability to flexibly adapt, even when situational demands are extreme. It has been furthermore argued that intermittent acute stress can foster a state of psychophysiological toughness associated, inter alia, with emotional stability, suppression of cortisol release and improved immune system function [20]. In conclusion, work rhythm that involves alternation between limited periods of high strain and sufficiently long phases of moderate load may foster behavioral and psychophysiological adjustment to stress, thereby facilitating the maintenance of health and wellbeing.
In addition to its clinical relevance, research on stress in crisis managers addresses the issue of professional performance. It has been well-established that performance in cognitive domains such as attention, memory, logical reasoning and decision-making varies according to the degree of psychophysiological activation, where optimal functional conditions are expected at midrange arousal, with both overarousal and underarousal accompanied by declines in performance [44]. The connection between stress and performance has been investigated, for instance, in the fields of high-risk industry, the military, and aviation [59,29,36]. Furthermore, medical performance appears to be compromised by acute stress. [37] showed that in paramedics experimental stress induced by a challenging scenario involving a human patient simulator reduced the accuracy of drug dosage calculations. Similarly, paramedics made more mistakes during patient care documentation under conditions of high vs. low simulated clinical stress [39]. Research on stress as a possible cause of impaired crisis management performance is still lacking. However, given the potential consequences of stress-related mistakes or incorrect decisions, for individual human lives and public safety, this issue is highly relevant. In the current study, a group of crisis managers from Tyrol (Austria) was compared with a matched control group comprised of managers drawn from other disciplines, in terms of self-reported stress and psychophysiological stress responses. Managers were chosen as a reference group to control for more general effects, which may arise due to the tenure of an executive position per se. In this way, possible group differences in the assessed parameters may be attributed to specific factors inherent in crisis management.
Participants were presented with multidimensional questionnaires quantifying perceived stress, resources enabling recuperation from burdensome events or stressful periods, and subjective health status. Furthermore, various experimental stressors were applied to investigate psychophysiological and emotional stress responses. These included short- and long-duration visual and acoustic stimuli resembling stressors specifically related to major incidents and crisis management, as well as non-specific emotional stressors. A mental arithmetic task was additionally employed in order to evoke cognitive stress. Psychophysiological response parameters comprised heart rate and electrodermal activity (EDA). While stress-related changes in heart rate occur due to alterations in the activity of the sympathetic and parasympathetic nervous systems, EDA constitutes a pure sympathetic measure [18,8]. In addition, the high frequency band of the heart rate variability (HRV) spectrum was also assessed. High frequency HRV is a well-established index of parasympathetic influences on heart activity (c.f. [7]). Acute and chronic stress is associated with a reduction in HRV, where a large database confirms the presence of low levels of high frequency HRV in physical and mental disease. Diminishment has been reported, for instance, in posttraumatic stress [60], anxiety disorders [41], depression [15] and physical conditions such as hypertension, cardiac disease or chronic pain [43,47,52]. Reduced HRV is furthermore linked to general morbidity and increased mortality [2].
This contribution constitutes the first controlled study on self-reported stress and psychophysiological stress reactivity in crisis managers. As such, to some extent it has to remain exploratory; definite predictions are therefore difficult to make. On one hand, the aforementioned research on paramedics and firefighters suggests increased stress and stress-related health problems in individuals working in disaster environments [1,5,31,24]. However, these data are not necessarily meaningful for crisis managers, because the respective professional groups clearly differ in their duties and professional roles. On the other hand, crisis managers commonly undergo a careful selection process, are highly trained and can resort to elaborate guidelines [54,56]. There specific professional condition may facilitate the development of flexible strategies to control stress and behaviorally and psychophysiologically adjust to the profound challenges of their role.
Methods
Participants
Thirty crisis managers (24 men, 6 women) participated in the study. The group was comprised of golden and silver commanders of institutions involved in the crisis management of major incidents. In their middle and higher management positions, these individuals were required to have staff and decision-making responsibilities, and furthermore to possess experience in the management of actual crises (and not merely exercises). The participants' mean duration of crisis management was 10.79 years (SD = 7.74 years), with involvement in an average in 73.77 operations (SD = 271.20 operations). Crisis managers currently involved in a crisis intervention were excluded. In order to recruit this group, the study was presented to the government of the Federal State of Tyrol (Austria), which established contacts with the Civil and Disaster Protection Tyrol, the Red Cross Kufstein and the Alpine Rescue Service Tyrol. The heads of these organisations received comprehensive information on the study; they all endorsed the participation of their crisis managers and invited them to do so via email or personal communication. Those who agreed to participate contacted the research team by phone. The control group included 30 mid- and high-level managers (23 men, 7 women) from the sectors of economy, industry, education and public administration. As with the crisis managers, these subjects were also required to operate in a leadership capacity and be responsible for staff. This group was recruited via large- and medium enterprises and public bodies. The exclusion criteria for both groups included any kind of serious physical disease or psychiatric disorder, as well as use of medication affecting the cardiovascular or nervous systems. Health status was assessed based on anamnestic interviews and a comprehensive medical questionnaire. Table 1 delineates the organizations and positions of all participants. Demographic data are given in Table 2. The groups did not differ significantly in age, work experience, educational level or body mass index (c.f. Table 2). The study was approved by the ethics committee of UMIT - University of Health Sciences, Medical Informatics and Technology; all participants provided written informed consent.
| Organisation | N (%) | Position | N (%) | |
| Crisis managers | ||||
| Civil defense | 11 (37%) | Operation controller | 18 (60%) | |
| Red Cross | 13 (43%) | Chief of the office | 6 (20%) | |
| Other organizations | ||||
| (e.g., emergency dispatch center, | 6 (20%) | Chief executive officer | 6 (20%) | |
| mountain rescue service) | ||||
| Control group | ||||
| Small and medium-sized | ||||
| enterprise (e.g., business consultancy, | 11 (37%) | Head of department | 12 (40%) | |
| IT service, architectural firm) | ||||
| Large-scale enterprise | 9 (30%) | Managing director | 8 (27%) | |
| (e.g., bank, pharmaceutical industry) | ||||
| Educational institution | ||||
| (e.g., elementary school, | 7 (23%) | President/director | 3 (10%) | |
| special school, university) | ||||
| Public administration | ||||
| (e.g., social assistance office, | 3 (10%) | Project manager | 4 (13%) | |
| municipal administration) | ||||
| Rector/vize-rector | 3 (10%) |
| Crisis managers | Control group | F[1, 58] | p | Partial $\mathbf{\eta^{2}}$ | |
| Age (years) | 43.00 (10.45) | 42.57 (10.05) | 0.03 | .87 | <.001 |
| Total work experience | |||||
| (years) | 22.83 (10.96) | 19.03 (11.31) | 1.75 | .19 | .03 |
| Time of education (years) | 15.67 (4.83) | 17.75 (3.88) | 3.39 | .07 | .06 |
| Body mass index (kg/m$^2$) | 25.27 (3.74) | 23.97 (3.33) | 2.01 | .16 | .03 |
Questionnaires
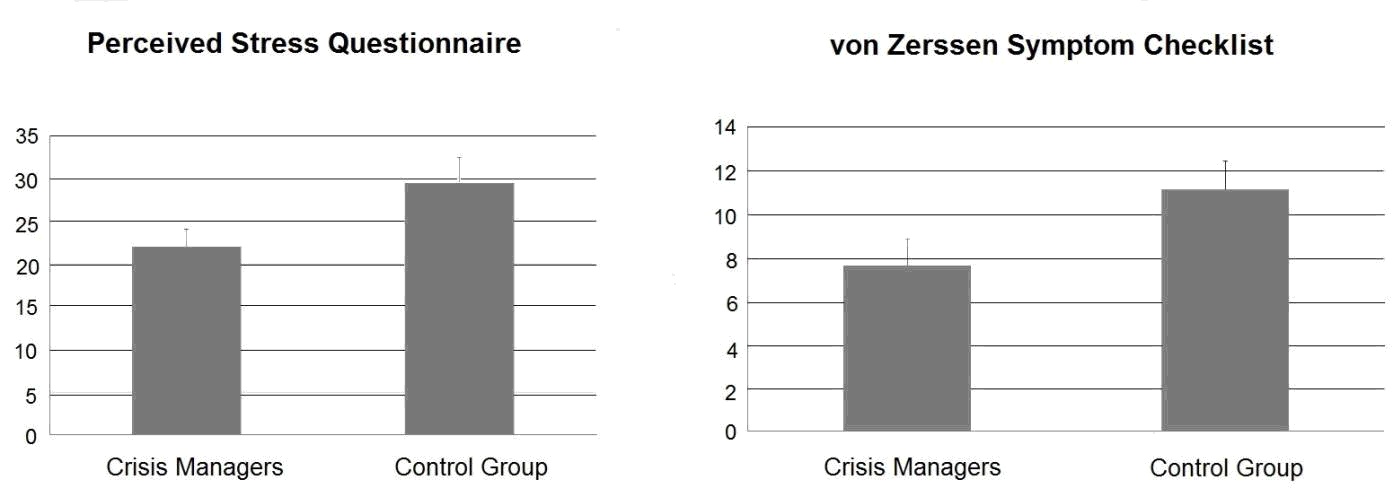
To determine self-reported stress, the German version of the Perceived Stress Questionnaire was applied [40]. This instrument aims to quantify currently perceived stress using four subscales each comprising five items. The Worries scale quantifies worries and anxious concern regarding the future, as well as feelings of desperation and frustration (possible range: 5-20); the Tension scale is concerned with agitation, fatigue and the inability to relax (possible range: 5-20); the Joy scale indexes positive feelings of joy, energy and security (possible range: 5-20). Finally, the Demands scale relates to perceived environmental stressors such as time pressure and overload (possible range: 5-20). In addition, a sum score is provided (possible range: 0-100). Joy scale items are inversely coded, such that higher values on all scales reflect increased stress.
The short version of the Questionnaire for Recuperation and Strain ([Erholungs-Belastungs-Fragebogen], EBF-24 A/3, Kallus, 1995) was also administered. This questionnaire estimates an individual's current recuperation-strain-balance; its 24 items refer to events inducing strain and those which facilitate recuperation, per the following 12 subscales: (1) General Strain (possible range: 0-12), (2) Emotional Strain (possible range: 0-12), (3) Social Strain (possible range: 0-12), (4) Unresolved Problems (possible range: 0-12), (5) Fatigue (possible range: 0-12), (6) Lack of Energy (possible range: 0-12), (7) Physical Problems (possible range: 0-12), (8) Success (possible range: 0-12), (9) Social Recreation (possible range: 0-12), (10) Physical Relaxation (possible range: 0-12), (11) General Content (possible range: 0-12) and (12) Sleep (possible range: 0-12). While higher values on scales 1 to 7 indicate increased levels of strain, higher values on scales 8 to 12 indicate the availability of recuperative and coping resources.
Subjective health status was assessed using the revised form of the von Zerssen Symptom Checklist ([Beschwerden-Liste], BL-R, [64]). This instrument is widely used in German speaking countries to quantify current burden with somatic complaints. The 20 items of the questionnaire include frequently experienced general symptoms (e.g., fatigue, tiredness) as well as more specific complaints (e.g., chest pain, nausea, insomnia). Higher values represent greater burden with bodily complaints (possible range: 0-60). In addition to these questionnaires, the demographic data sheet included questions about basic features of health behavior, i.e. smoking status, alcohol consumption and physical exercise.
Experimental Stress Induction
Three types of stimuli were used to experimentally evoke acute emotional and cognitive stress. Participants were initially presented with images from the International Affective Picture System (IAPS) [35], a picture viewing paradigm popular in emotion and stress research. The following three image categories were applied (15 images per category1 ): (1) images resembling stressors related to major incidents (e.g., injuries and mutilations), (2) images representing general (non-specific) stressors (e.g., threatening or anxiety-related situations), and (3) pleasant stimuli (e.g., positive social situations and erotic images). The pleasant images served as a control condition allowing investigation of a possible group difference in general emotional responsiveness. Normative ratings of stimuli on the arousal and valence dimensions were as follows (Lang et al., 1997): crisis-related images, arousal M = 6.24, SD = 0.64, valence M = 7.08, SD = 0.35; non-specific stress images, arousal M = 6.49, SD = 0.41, valence M = 6.39, SD = 0.65; pleasant images, arousal M = 6.17, SD = 0.83, valence M = 1.81, SD = 0.56 (higher values denote higher arousal and more negative valence.) The images were presented in a pseudorandom order, where stimuli of all three categories (crisis-related stressors, non-specific stressors, pleasant images) were intermixed. Stimulus duration was 5 s each, with interstimulus intervals (white cross on the screen) ranging between 8 and 12 s.
Two acoustic stressors were additionally applied. First, a series of noises was compiled based on stimuli taken from the International Affective Digitized Sounds database (IADS) [11]2 .2 Selected noises included a human scream, the take-off and landing of a helicopter and a ringing phone, all of which are purportedly associated with major incidents or crisis management. The three sounds were repeatedly presented in a pseudorandom order over 1 min. Normative ratings were as follows [11]: arousal M = 6.48, SD = 1.17, valence M = 3.59, SD = 1.97. As an non-specific acoustic stressor, a piece of self-programmed, non-melodic synthesizer music was used. Each of the acoustic stressors was presented for 1 min via earphones (sound pressure level 59 - 63 dB). The stimulation phases were preceded by 1 min resting periods. Participants rated their affective experience elicited by the emotional stimuli (IAPS pictures, IADS noises), in terms of arousal and valence, using the Self-Assessment Manikin scales (SAM) [10] (possible range of both scales: 1-9). For this purpose, IAPS stimuli were repeated in the same sequence following the initial presentation. Evaluation of IADS noises was accomplished directly after they were presented. The Montreal Imaging Stress Task (MIST) [19] was applied as a cognitive stressor. The MIST requires resolving arithmetic problems under time pressure. The problems are presented in conjunction with an unpleasant noise, where the intensity of the noise increases until the correct solution is entered. The total task time was 3 min, preceded by a 1 min resting period and followed by a 2 min recovery phase. All visual stimuli were displayed on a 19 inch monitor (distance between subject and monitor approx. 1 m). Presentation of the IAPS and IADS stimuli was controlled using the Presentation software package (ver. 17.1, Neurobehavioral Systems, USA). The order of task presentation was as follows (identical order in all participants): 1. visual stimuli; 2. crisis-related acoustic stressor; 3. non-specific acoustic stressor; and 4. cognitive stressor.
Psychophysiological Recordings
Heart rate and electrodermal activity (EDA) were assessed using a Biopac system (MP 150, Biopac Systems Inc., USA). Heart rate was taken using ECG, which was recorded from two electrodes placed at the right mid-clavicle and lowest left rib. EDA electrodes were attached to the third and fourth fingers of the non-dominant hand. All data were digitized at a sampling rate of 1000 Hz.
Prior to the presentation of the stimuli, recordings were accomplished during resting conditions for 10 min. For this part of the procedure, the participants were asked to fixate upon a white cross, which was presented in the center of a black computer screen. Subjects were requested not to drink alcohol or beverages containing caffeine for at least 2 h prior to the experimental session.
Data Analysis
To aggregate the psychophysiological data, the AcqKnowledge (ver. 4, Biopac Systems Inc., USA) and KARDIA [49] software packages were employed. In a first step, values of heart cycle duration - defined as the RR interval - were computed from the raw ECG. The ECG data was visually screened, and artifacts were corrected by linear interpolation. Subsequently, the beat-to-beat values were transformed to time-based data with a sample rate of 2 Hz. The EDA data was resampled at the same frequency. Mean heart rate values were computed for the 10 min resting period, during which high frequency HRV was also obtained. To this end, the software Kubios HRV (ver. 2) [46], was employed, which follows Task Force (1996) cite{task1996heart} guidelines. HRV was derived from the series of RR intervals by means of Fast-Fourier-Transformation (extraction through a Hamming window). Spectral power density was expressed in absolute units. High frequency HRV was indexed by spectral power density in the frequency range between 0.15–0.40 Hz.
To quantify psychophysiological responses to the presentation of stressors, (absolute) changes from baseline were computed for heart rate and EDA. Baseline duration was set at 3 s for the IAPS stimuli, and 5 s for the acoustic stimuli and the MIST, respectively. For the IAPS stimuli, the data was averaged across the 15 images of each category. Peak amplitudes of the psychophysiological responses were computed for all stressors. Therefore, maximum changes were determined in specific response intervals, defined according to visual inspection of the data. Regarding the IAPS stimuli, this time window comprised the first 5 s after stimulus onset for heart rate and EDA. As the acoustic and cognitive stressors elicited the strongest heart rate and EDA modulations during the initial stimulation phase, peak amplitudes were determined in the first 10 seconds following stimulus onset for both acoustic stimuli and in the first 15 seconds for the MIST.
In addition, stress-induced changes in high frequency HRV were quantified for the MIST. As the execution of the task involved relatively long recording periods (1 min baseline, 3 min task execution, 2 min recovery), which are recommended for reliable determination of HRV [7], this stressor was the most appropriate for this purpose. As a main instrument of statistical analysis, a MANOVA was computed with study group (crisis managers vs. control group) as a between-subjects factor. Dependent variables comprised the demographic and questionnaire data as well as the psychophysiological indices. Data analysis showed that crisis managers engaged in markedly more physical exercise compared to the control group. To test whether physical exercise moderated group differences in the remaining dependent variables, a second MANOVA was computed with physical exercise (hours/week) used as a covariate. To evaluate changes in HRV during execution of the MIST, an ANOVA was conducted with study group as between-subjects factor and condition (baseline vs. task execution vs. recovery) as a within-subjects factor. The alpha-level was set at .05 for all analyses.
Results
Multivariate testing revealed a significant effect of group (F[38, 21] = 2.70, p = .009, Partial Eta Squared = .83). According to univariate testing, crises managers exhibited a lower total score of the Perceived Stress Questionnaire than the control group (F[1, 58] = 4.39, p = .041, Partial Eta Squared = .070) (c.f. Figure 1). Regarding the Questionnaire for Recuperation and Strain, crises managers showed lower scores on the Social Strain and Physical Problems scales, and higher scores on the Social Recreation scale (c.f. Table 3). In addition, lower values for crisis managers vs. the control group were observed on the von Zerssen Symptom Checklist F[1, 58] = 4.47, p = .039, Partial Eta Squared = .072) (c.f. Figure 1).
| Crisis managers | Control group | F[1,58] | p | Partial $\mathbf{\eta^{2}}$ | |
| Perceived Stress | |||||
| Questionnaire | |||||
| Worries | 11.78 (11.30) | 16.67 (12.84) | 2.45 | .12 | .04 |
| Tension | 21.33 (12.67) | 26.44 (16.47) | 1.82 | .18 | .03 |
| Joy | 82.44 (14.38) | 77.11 (16.11) | 1.83 | .18 | .03 |
| Demands | 37.11 (17.65) | 52.22 (51.08) | 2.35 | .13 | .04 |
| Questionnaire for | |||||
| Recuperation and Strain | |||||
| General Strain | 0.32 (0.40) | 0.52 (0.76) | 1.62 | .21 | .03 |
| Emotional Strain | 0.55 (0.55) | 0.75 (0.70) | 1.51 | .22 | .03 |
| Social Strain | 0.80 (0.58) | 1.25 (0.87) | 5.56 | .02 | .03 |
| Unresolved Problems | 1.72 (1.01) | 1.93 (1.30) | 0.52 | .48 | .01 |
| Fatigue | 0.32 (0.40) | 0.52 (0.67) | 1.62 | .21 | .03 |
| Lack of Energy | 1.12 (0.63) | 0.98 (0.84) | 0.49 | .49 | .01 |
| Physical Problems | 0.70 (0.43) | 1.30 (1.18) | 6.87 | .01 | .11 |
| Success | 3.48 (0.97) | 3.37 (1.16) | 0.18 | .67 | <.01 |
| Social Recreation | 3.98 (0.83) | 3.30 (1.52) | 4.67 | .04 | .08 |
| Physical Relaxation | 4.47 (0.93) | 4.08 (1.23) | 1.87 | .18 | .03 |
| General Content | 4.82 (0.71) | 4.55 (0.82) | 1.80 | .19 | .03 |
| Sleep | 5.03 (1.06) | 5.12 (0.93) | 0.11 | .75 | <.01 |
| Crisis managers | Control group | F[1, 58] | p | Partial $\mathbf{\eta^{2}}$ | |
| Self-Assessment Manikin | |||||
| Crisis-related images | |||||
| Valence | 6.52 (1.51) | 7.48 (0.78) | 9.64 | <.01 | .14 |
| Arousal | 3.71 (1.44) | 5.15 (1.55) | 13.84 | <.01 | .19 |
| Non-specific stress images | |||||
| Valence | 6.49 (1.56) | 6.99 (0.87) | 2.35 | .13 | .04 |
| Arousal | 3.51 (1.56) | 3.01 (0.87) | 2.35 | .13 | .04 |
| Pleasant images | |||||
| Valence | 2.93 (1.61) | 2.94 (1.44) | <.01 | .98 | <.01 |
| Arousal | 3.64 (1.75) | 4.41 (1.39) | 3.61 | .06 | .06 |
| Crisis-related noises | |||||
| Valence | 7.83 (1.39) | 7.97 (1.45) | 0.13 | .72 | <.01 |
| Arousal | 3.63 (2.06) | 3.00 (1.68) | 1.70 | .20 | .03 |
| Response amplitudes | |||||
| EDA ($\mathbf{\mu\textrm{S}}$) | |||||
| IAPS: crises-related stress | 0.05 (0.07) | 0.08 (0.14) | 1.12 | .29 | .02 |
| IAPS: non-specific stress | 0.04 (0.05) | 0.08 (0.10) | 4.63 | .04 | .07 |
| IAPS: positive stimuli | 0.04 (0.07) | 0.05 (0.01) | 0.03 | .86 | <.01 |
| Acoustic: crises-related stress | 0.82 (0.59) | 1.54 (1.15) | 9.48 | <.01 | .14 |
| Acoustic: non-specific stress | 0.40 (0.42) | 0.85 (0.78) | 7.74 | <.01 | .12 |
| MIST | 0.93 (0.73) | 1.38 (0.85) | 5.00 | .03 | .08 |
| Heart rate (beats/min) | |||||
| IAPS: crises-related stress | -1.21 (0.81) | -2.04 (2.04) | 4.30 | .04 | .07 |
| IAPS: non-specific stress | -1.22 (0.85) | -2.08 (1.85) | 5.37 | .02 | .09 |
| IAPS: positive stimuli | -1.91 (1.17) | -2.40 (1.43) | 2.14 | .15 | .04 |
Figure 2 presents the modulations in EDA and heart rate elicited by the IAPS images depicting crisis-related and non-specific stressors. EDA increased during picture presentation and peaked between the third and fourth second after stimulus onset. For both picture categories amplitudes were lower in crisis managers than in the control group. Heart rate decelerated during the early stimulation phase and subsequently increased above baseline level. The magnitude of the deceleration component was smaller in crisis managers for both picture categories. The EDA responses to the acoustic stressors are displayed in Figure 3. Crisis-related IADS sounds, and non-specific aversive noises, triggered a steep increase in the signal, which reached its maximum five seconds after stimulus onset and returned to baseline around second 10. A similar pattern was observed during execution of the MIST (c.f. Figure 4), where the maximum occurred slightly later. The initial responses were weaker in crisis managers than in controls for both acoustic stressors as well as the MIST.
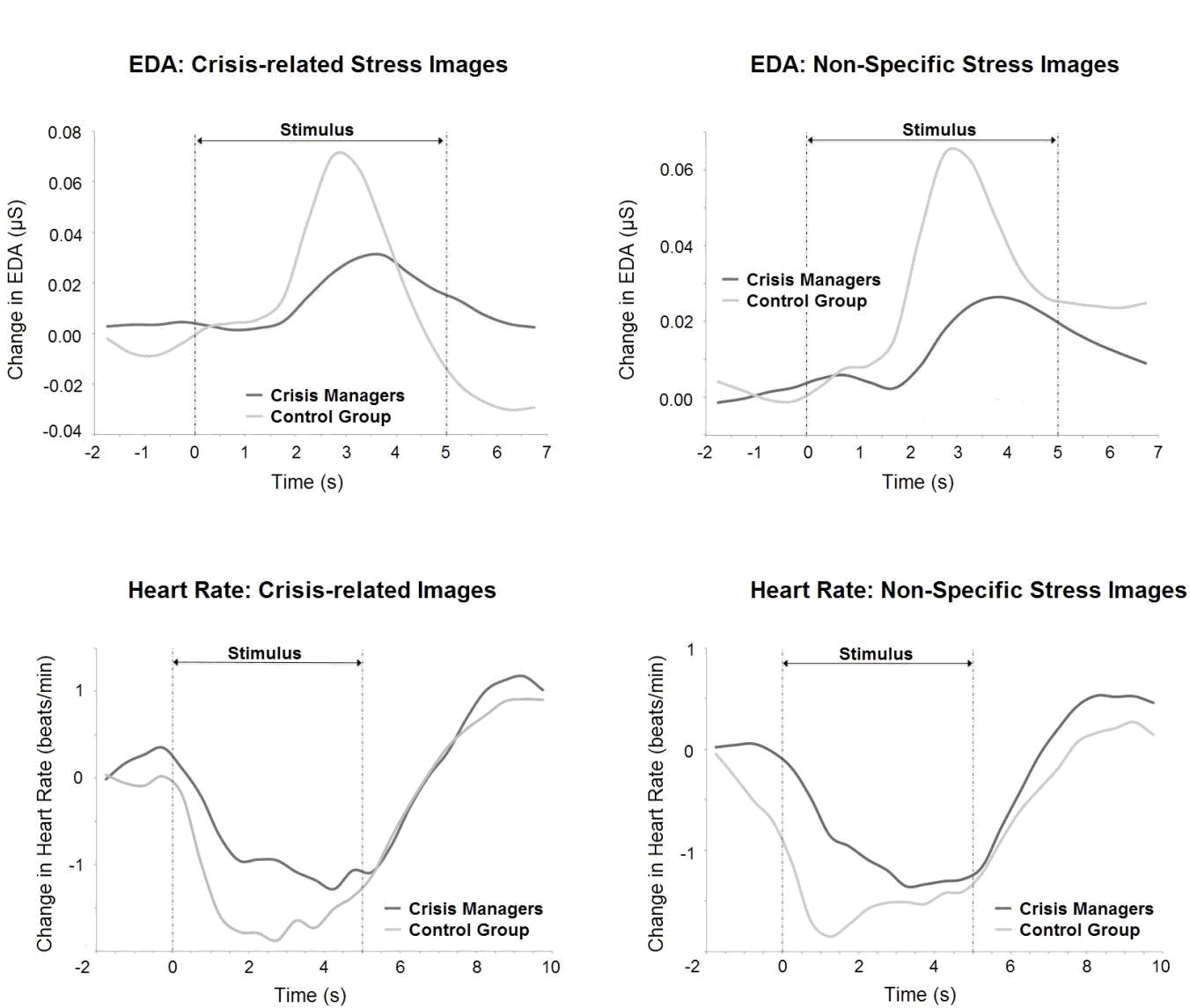
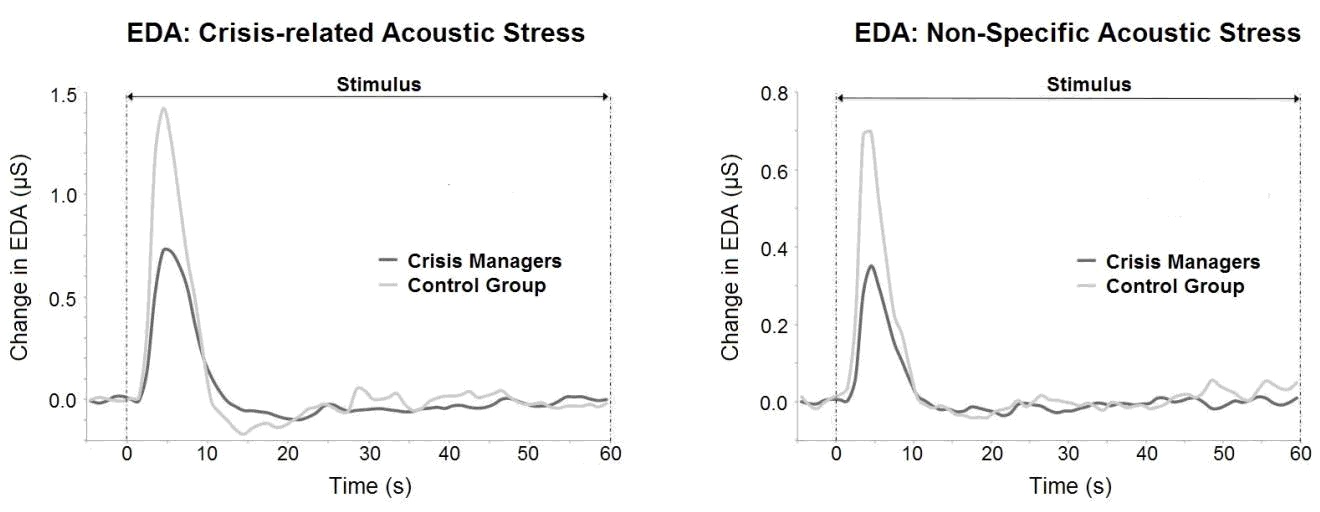
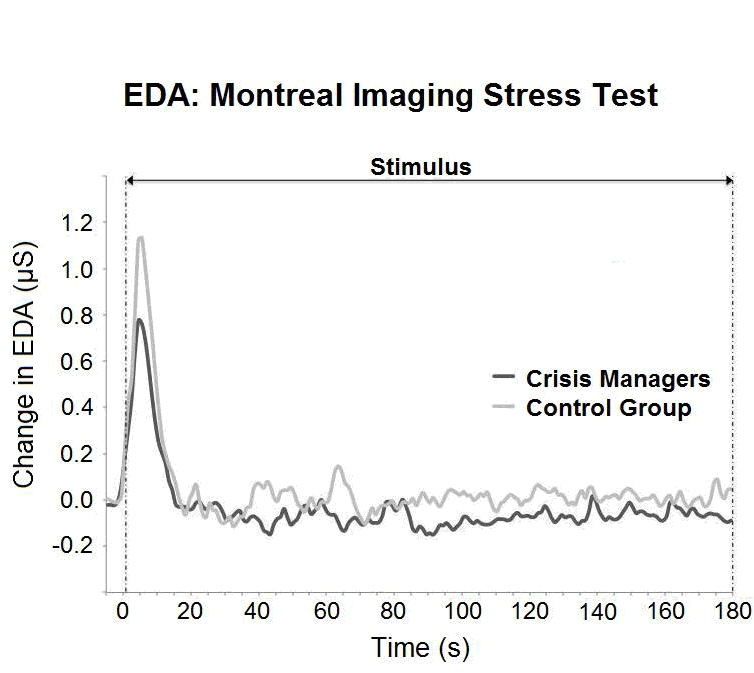
The numeric amplitude values of the EDA and heart rate responses are displayed in Table 3. With respect to EDA, group differences reached significance for the IAPS pictures depicting non-specific stressors, for both acoustic stressors, as well as for the MIST. The amplitude of heart rate decline was significantly reduced in crisis managers, for the crisis-related and non-specific stressor pictures. No significant group differences emerged for the positive pictures, nor for heart rate responses to the acoustic and cognitive stressors (data not shown). Analysis of high frequency HRV for the MIST revealed, in both groups, a decrease during task execution and an increase during the recovery period (crisis managers: baseline M = 610.37 ms2, SD = 1143.94 ms2, task execution M = 381.32 ms2, SD = 650.06 ms2, recovery M = 626.16 ms2, SD = 1174.47 ms2; control group: baseline M = 559.61 ms2, SD = 870.42 ms2, task execution M = 465.07 ms2, SD = 700.23 ms2, recovery M = 566.55 ms2, SD = 930.99 ms2). In the ANOVA this was reflected by a main effect of condition (F[2, 116] = 3.77, p = .026, partial Eta squared = .061). However, neither the group effect, nor the interaction between both factors, reached significance (group: F[1, 58] = 0.002, p = .97, partial Eta squared <.001; interaction: F[2, 116] = 0.65, p = .53, partial Eta squared = .011).
Discussion
In the present study, a group of Austrian crisis managers was compared with managers from other disciplines on measures of self-reported stress and recuperative resources, in addition to self-reported health status and psychophysiological and emotional responses to experimental stressors. Crisis managers exhibited a lower sum score on the Perceived Stress Questionnaire, suggesting an overall lower stress burden. Results concerning the Questionnaire for Recuperation and Strain furthermore point toward a more positive recuperation-strain-balance in crisis managers, indexed by lower scores on the Social Strain and Physical Problems scales and higher scores on the Social Recreation scale. The finding of reduced somatic complaints is corroborated by the lower values on the von Zerssen Symptom Checklist.
The self-report data are complemented by evidence of diminished psychophysiological reactivity to experimental stressors in crisis managers. Specifically, they were characterized by smaller heart rate modulations when exposed to images depicting crisis-related stressors and non-specific threatening situations, as well as weaker EDA responses to non-specific threatening images. Moreover, initial EDA increases during a series of noises associated with crisis situations, as well as non-specific aversive sounds, were markedly lower in crises managers than in controls. Finally, crisis managers exhibited reduced EDA responses during cognitive stress induced by the MIST.
The smaller increases in skin conductance observed in crisis managers indicate lower stress-related sympathetic nervous system activation [18]. It is important to note that the reduced EDA reactivity was not restricted to stressors specifically associated with disaster scenarios and crisis management. Instead, the lower amplitudes elicited by non-specific aversive cues and the cognitive stressor support the notion of there being generally reduced sympathetic reactivity during stress from various sources. On the other hand, study groups did not differ in their EDA responses to pleasant images, suggesting that the crisis managers' lower signal increases were not due to generally blunted autonomic responsiveness. However, that the group difference in EDA reactions to crisis-related images also failed to reach significance should not be overlooked. In the entire sample, EDA modulations were far weaker for the visual stimuli than for both the noise series and the cognitive stressor. The latter conditions were apparently more capable of eliciting sympathetic activation, thereby more clearly differentiating the study groups. It is certainly noteworthy that crisis managers' average initial responses to both acoustic stressors were only approximately half as strong as those of the controls.
The pattern of heart rate modulation during presentation of the crisis-related and non-specific threatening images represents the typical response to affective stimuli of negative valence [12]. The initial heart rate deceleration is believed to relate to orientation toward the stimulus and heightened sensory processing [12]. The smaller amplitude of the heart rate decrease exhibited by crisis managers while viewing the pictures may therefore reflect a reduction in the attentional and sensory processing resources devoted to crisis-related and non-specific aversive cues. In addition, crisis managers experienced less unpleasantness and arousal in response to the crisis-related images. This may be due to habituation following repeated exposure to disaster environments, which can be viewed as an adaptive coping mechanism facilitating behavioral adjustment to these highly challenging situations.
The reduction in high frequency HRV during execution of the MIST reflects parasympathetic withdrawal, which is commonly elicited by conditions of acute stress [7]. Reductions in heart rate variability have been observed during exposure to various experimental stressors, including cognitive load (e.g., [22,21,53]. However, the study groups did not differ in the magnitude of stress-induced HRV modulation. It may therefore be concluded that the crisis managers' reduced physiological reactivity during cognitive activation was confined to the sympathetic system. In addition, no significant group differences emerged in HRV recorded at rest. High frequency HRV during resting state is a well-established risk marker of numerous physical and mental disorders, as well as a predictor of general morbidity [43,2,60,15]. The present data therefore does not support the view that there is a generally elevated health risk associated with the duties of crisis management.
Several factors could account for the superior subjective health, lower self-reported stress and reduced psychophysiological stress reactivity of the crisis managers. First, greater interpersonal resources, to facilitate coping with crises-related burden and general occupational stressors should be considered. This is supported by the higher scores on the Social Recreation scale of the Questionnaire for Recuperation and Strain, which aims to quantify the presence of positive social contacts associated with pleasant feelings and easing of tension (Kallus, 1995). Moreover, crisis managers' lower scores on the Social Strain scale suggest a reduced burden from conflicts, and a more positive perception of the social environment. Social support and a positive social network undoubtedly represent powerful recuperative resources, with empirical evidence confirming that social support reduces stress and facilitates coping [61]. The positive effects of social support on physical and mental health are also beyond question (e.g., [62,51,48]). In the present context it is also notable that social support has been shown to diminish psychophysiological reactivity to experimental stressors (e.g., [58,61]).
As mentioned in the Introduction section, psychological flexibility may furthermore contribute to improved stress-resistance in crisis managers. Their working conditions, involving significant but time-limited stressor exposure and longer phases of moderate strain, may foster greater flexibility in behavioral, cognitive and energetic adjustments, thereby conferring health benefits [33]. In terms of “stress inoculation”, confrontation with intermittent, strong stressors may furthermore promote psychophysiological toughness and resilience [20]. In contrast, more constant exposure to relatively uniform stressors, which may be more typical of the conditions under which managers in other occupational sectors operate, may be less helpful with respect to the acquisition of coping flexibility and toughness. In some crisis managers, a tendency to pursue high levels of stimulation and limit experiences, i.e. sensation seeking [65], may also play a role.
The possible contribution of health behaviors, in particular physical activity, to group differences should also be discussed. Regular exercise is known to increase stress tolerance [28], improve affective wellbeing [50], and confer benefits to mental and physical health (e.g., [23]). Various studies have furthermore demonstrated that higher levels of physical exercise and fitness are associated with reduced psychophysiological stress reactivity (e.g., [26]). The crisis managers investigated did indeed report almost twofold more physical exercise than the control group. However, the role of this variable in moderating group differences is challenged by the finding that almost all of the outcome measures remained significant after its inclusion as a covariate in the MANOVA. The group effect for physical health, assessed using the von Zerssen Symptom Checklist, disappeared when physical exercise was held constant, which is put into perspective by the finding that the difference in the Physical Problems scale of the Questionnaire for Recuperation and Strain remained significant. However, it should be noted that habitual health behaviors were assessed only approximately, by two questions referring to the time per week that participants spent on sports and the days per week on which they consumed alcohol. In future studies, it would be useful to include a more comprehensive health behavior assessment, using a validated psychometric instrument. Moreover, in addition to physical exercise, physical fitness, for example in terms of physical working capacity or maximum oxygen consumption, should also be taken into consideration (c.f. [3]).
Moreover, processes of professional selection should be considered in the present findings. The work history of many crisis managers includes substantial activity within rescue services, where they are repeatedly exposed to disaster environments and associated stressors. It may be that it is predominantly these types of individuals who reach leading positions in the field, by demonstrating the ability to efficiently cope with such burdens. Successful acquisition of psychological flexibility may also be of relevance in this selection process. The investigated sample was characterized by a relatively high level of professional experience, i.e. approximately 11 years of crisis management and 23 years' total work experience. Therefore, a “survivor effect” cannot be ruled out, in which only those individuals who are more stress-resistant continue to work in crisis management for such a long period of time; those who are less resilient are more likely to have changed jobs earlier in their careers. As such, the results may be applicable specifically to senior crisis managers, and may not necessarily generalize to those with less experience.
It should not be overlooked that some studies have suggested greater strain, and reduced wellbeing, in other professionals working in disaster environments, particularly paramedics and rescue workers [1,5,31]. By definition, crisis managers must be regarded as a specific occupational group that clearly differs from rescue personnel, in terms of their duties and particular role within their team. It has been demonstrated in other occupational fields that holding a leadership position does not confer increased strain and health risk, but rather that perceived occupational stress is inversely related to status in professional hierarchy [42,57]. This may be explained within the framework of the classical job demand-control model [32], in which mental strain due to demanding work is reduced if an individual can exert greater job control in terms of decisional latitude and scope for action. To further clarify this issue, our research approach could be extended in future studies. While in the present design crisis management was contrasted with other leading positions, comparisons between crisis managers and action forces or medical personnel would allow for assessment of differences in self-reported stress and psychophysiological stress responses associated with different emergency aid roles and functions: the contributions of specific occupational and organizational factors (e.g., command structure, allocation of discretionary competencies and management responsibilities, workload or job content) to stress levels could be systematically analyzed.
By definition, the present findings primarily reflect only crisis managers in Austria and cannot be generalized to other countries. Due to the limited number and availability of local crisis managers, the sample employed was relatively small. This is particularly relevant to the self-report measures, where a larger sample size may have enabled a more efficient investigation of the specific pattern of stress components and psychosocial resources. Moreover, even though the study groups did not differ significantly in terms of relevant demographics, a case-control design specifically matching each crisis manager to a non-crisis manager for these variables may have been superior to the one used presently. As a further limitation, possible distortion of the self-report data due to demand effects of the questionnaires may be taken into account. It may be that some crisis managers' self-concept includes, for example, particularly high stress resistance and recuperative resources. These capacities may be more inherent to the occupational image of crisis managers compared to leaders in other fields. It therefore is possible that a part of this group exhibited a response tendency toward presenting themselves as particularly robust and resilient. Selection bias in the recruitment of participants should also be taken into account. Because only a subgroup of crisis managers, who were invited to participate by their supervisors, responded to this offer, it cannot be ruled out that those with a low subjective stress burden and pronounced resistance were more likely to participate.
As the first systematic analysis of stress in crisis managers, this study revealed evidence of lower stress burden, a more positive recuperation-strain-balance and improved self-rated health status. Moreover, crisis managers' reduced autonomic reactivity to both crisis-related and non-specific stressors and cognitive challenge point towards elevated bodily stress resistance. These data underline crisis managers' increased behavioral and psychophysiological adjustment to the extreme demands of their vocation. In addition to its importance for the conservation of physical and mental health, improved stress tolerance may also reduce vulnerability to stress-related performance decline, thereby helping to ensure adequate preparedness to major incidents and maintenance of public security.
Acknowledgments
The study was supported by the European Commission (project PsyCris, FP7-SEC-2012-1).
Compliance with Ethical Standards
Conflict of interest
A. Janka, C. Adler, L. Fischer, P. Perakakis, P. Guerra and S. Duschek declared that they have no conflict of interest.
Human and animal rights and Informed Consent
All procedures followed were in accordance with ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
References
- Alexander, D. A. , & Klein, S. (2001). Ambulance personnel and critical incidents. The British Journal of Psychiatry, 178(1), 76–81. doi:10.1192/bjp.178.1.76
- Almoznino-Sarafian, D. , Sarafian, G. , Zyssman, I. , Shteinshnaider, M. , Tzur, I. , Kaplan, B.- Z. &ldots;Gorelik, O. (2009). Application of HRV-CD for estimation of life expectancy in various clinical disorders. European Journal of Internal Medicine, 20(8), 779–783. doi:10.1016/j.ejim.2009.08.006
- American College of Sports Medicine. (2013). ACSM's guidelines for exercise testing and prescription. Lippincott Williams & Wilkins.
- Beaton, R. , Murphy, S. , & Pike, K. (1996). Work and nonwork stressors, negative affective states, and pain complaints among firefighters and paramedics. International Journal of Stress Management, 3(4), 223–237. doi:10.1017/S1049023X00040218
- Bennett, P. , Williams, Y. , Page, N. , Hood, K. , & Woollard, M. (2004). Levels of mental health problems among uk emergency ambulance workers. Emergency Medicine Journal, 21(2), 235–236. doi:10.1136/emj.2003.005645
- Berger, W. , Coutinho, E. S. F. , Figueira, I. , Marques-Portella, C. , Luz, M. P. , Neylan, T. C. &ldots;Mendlowicz, M. V. (2012). Rescuers at risk: a systematic review and meta-regression analysis of the worldwide current prevalence and correlates of ptsd in rescue workers. Journal of Social psychiatry and psychiatric epidemiology, 47(6), 1001–1011. doi:10.1007/s00127-011-0408-2
- Berntson, G. G. , Bigger, J. T. , Eckberg, D. K. , Grossman, P. , Kaufmann, P. G. , Malik, M. &ldots;van der Molen, M. W. (1997). Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology, 34, 623–648. doi:10.1111/j.1469-8986.1997.tb02140.x
- Berntson, G. G. , Quigley, K. S. , & Lozano, D. (2007). Cardiovascular psychophysiology. In Cacioppo, J.T., Tassinary, L.G., & Berntson, G.G. (Eds.). Handbook of psychophysiology.
- Bonanno, G. A. , Papa, A. , Lalande, K. , Westphal, M. , & Coifman, K. (2004). The importance of being flexible the ability to both enhance and suppress emotional expression predicts long-term adjustment. Psychological Science, 15(7), 482–487. doi:10.1111/j.0956-7976.2004.00705.x
- Bradley, M. M. , & Lang, P. J. (1994). Measuring emotion: the self-assessment manikin and the semantic differential. Journal of behavior therapy and experimental psychiatry, 25(1), 49–59. doi:10.1016/0005-7916(94)90063-9
- Bradley, M. M. , & Lang, P. J. (2007a). The International Affective Digitized Sounds (2nd; IADS-2): Affective ratings of sounds and instruction manual. University of Florida, Gainesville, FL, Tech. Rep. B-3.
- Bradley, M. M. , & Lang, P. J. (2007b). Emotion and Motivation. In Cacioppo, J.T., Tassinary, L.G., & Berntson, G.G. (Eds.). Handbook of Psychophysiology.
- Brannon, L. , Feist, J. , & Updegraff, J. (2007). Health psychology: An introduction to behavior and health. Cengage Learning.
- Brown, J. , Mulhern, G. , & Joseph, S. (2002). Incident-related stressors, locus of control, coping, and psychological distress among firefighters in Northern Ireland. Journal of Traumatic Stress, 15(2), 161–168. doi:10.1023/A:1014816309959
- Bylsma, L. M. , Salomon, K. , Taylor-Clift, A. , Morris, B. H. , & Rottenberg, J. (2014). RSA Reactivity in Current and Remitted Major Depressive Disorder. Psychosomatic medicine, 76(1), 66. doi:10.1097/PSY.0000000000000019
- Critical Response in Security and Safety Emergencies. (2011). Retrieved from http://www.2020 horizon. com/CRISYS-Critical-Response-in-Security-and-Safety-Emergencies%28CRISYS%29-s5246.html.
- Cukor, J. , Wyka, K. , Mello, B. , Olden, M. , Jayasinghe, N. , Roberts, J. &ldots;Difede, J. (2011). The longitudinal course of PTSD among disaster workers deployed to the World Trade Center following the attacks of September 11th. Journal of Traumatic Stress, 24(5), 506–514. doi:10.1002/jts.20672
- Dawson, M. E. , Schell, A. M. , & Filion, D. L. (2007). The electrodermal system. In Cacioppo, J.T., Tassinary, L.G., & Berntson, G.G. (Eds.). Handbook of psychophysiology.
- Dedovic, K. , Renwick, R. , Mahani, N. K. , Engert, V. , Lupien, S. J. , & Pruessner, J. N. (2005). The Montreal Imaging Stress Task: using functional imaging to investigate the effects of perceiving and processing psychosocial stress in the human brain. Journal of psychiatry & neuroscience: JPN, 30(5), 319.
- Dienstbier, R. A. (1989). Arousal and physiological toughness: implications for mental and physical health. Psychological review, 96(1), 84.
- Duschek, S. , Muckenthaler, M. , Werner, N. , & Reyes del Paso, G. A. (2009). Relationships between features of autonomic cardiovascular control and cognitive performance. Biological psychology, 81(2), 110–117. doi:10.1016/j.biopsycho.2009.03.003
- Duschek, S. , Werner, N. , Kapan, N. , & Reyes del Paso, G. A. (2008). Patterns of cerebral blood flow and systemic hemodynamics during arithmetic processing. Journal of Psychophysiology, 22(2), 81–90. doi:10.1027/0269-8803.22.2.81
- Dylewicz, P. , Borowicz-Bienkowska, S. , Deskur-Smielecka, E. , Kocur, P. , Przywarska, I. , & Wilk, M. (2005). Value of exercise capacity and physical activity in the prevention of cardiovascular diseases – brief review of the current literature. Journal of Public Health, 13(6), 313–317. doi:10.1007/s10389-005-0127-9
- Essex, B. , & Scott, L. B. (2008). Chronic stress andassociated coping strategies among volunteer ems personnel. Prehospital Emergency Care, 12(1), 69–75. doi:10.1080/10903120701707955
- Fliege, H. , Rose, M. , Arck, P. , Levenstein, S. , & Klapp, B. (2001). Validierung des “Perceived Stress Questionnaire”(PSQ) an einer deutschen Stichprobe. Diagnostica, 47(3), 142–152. doi:10.1026//0012-1924.47.3.142
- Forcier, K. , Stroud, L. R. , Papandonatos, G. D. , Hitsman, B. , Reiches, M. , Krishnamoorthy, J. , & Niaura, R. (2006). Links between physical fitness and cardiovascular reactivity and recovery to psychological stressors: A meta-analysis. Health Psychology, 25(6), 723. doi:10.1037/0278-6133.25.6.723
- Guha-Sapir, D. , Vos, F. , Below, R. , & Penserre, S. (2012). Annual disaster statistical review 2011: the Numbers and Trends (Tech. Rep.). UCL. doi:10.1097/PSY.0b013e318148c4c0
- Hamer, M. , & Steptoe, A. (2007). Association between physical fitness, parasympathetic control, and proinflammatory responses to mental stress. Psychosomatic medicine, 69(7), 660–666.
- Harris, W. C. , Hancock, P. , & Harris, S. C. (2005). Information processing changes following extended stress. Military Psychology, 17(2), 115. doi:10.1207/s15327876mp1702_4
- Hoffman, B. M. , Babyak, M. A. , Craighead, W. E. , Sherwood, A. , Doraiswamy, P. M. , Coons, M. J. , & Blumenthal, J. A. (2011). Exercise and pharmacotherapy in patients with major depression: one-year follow-up of the smile study. Psychosomatic Medicine, 73(2), 127. doi:10.1097/PSY.0b013e31820433a5
- Kalemoglu, M. , & Keskin, O. (2006). Burnout syndrome at the emergency service. Scand J Trauma Resusc Emerg Med, 14, 37–40.
- Karasek Jr, R. A. (1979). Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative science quarterly, 24, 285–308.
- Kashdan, T. B. , & Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clinical psychology review, 30(7), 865–878. doi:10.1016/j.cpr.2010.03.001
- Klaperski, S. , von Dawans, B. , Heinrichs, M. , & Fuchs, R. (2014). Effects of a 12-week endurance training program on the physiological response to psychosocial stress in men: a randomized controlled trial. Journal of behavioral medicine, 37(6), 1118–1133.
- Lang, P. J. , Bradley, M. M. , & Cuthbert, B. N. (1997). International affective picture system (IAPS): Technical manual and affective ratings. NIMH Center for the Study of Emotion and Attention..
- LeBlanc, V. R. (2009). The effects of acute stress on performance: implications for health professions education. Academic Medicine, 84(10), S25–S33.
- LeBlanc, V. R. , MacDonald, R. D. , McArthur, B. , King, K. , & Lepine, T. (2005). Paramedic performance in calculating drug dosages following stressful scenarios in a human patient simulator. Prehospital Emergency Care, 9(4), 439–444. doi:10.1080/10903120500255255
- LeBlanc, V. R. , Regehr, C. , Birze, A. , King, K. , Scott, A. K. , MacDonald, R. , & Tavares, W. (2011). The association between posttraumatic stress, coping, and acute stress responses in paramedics. Traumatology, 17(4), 10. doi:10.1177/1534765611429078
- LeBlanc, V. R. , Regehr, C. , Tavares, W. , Scott, A. K. , MacDonald, R. , & King, K. (2012). The impact of stress on paramedic performance during simulated critical events. Prehospital and disaster medicine, 27(04), 369–374. doi:10.1017/S1049023X12001021
- Levenstein, S. , Prantera, C. , Varvo, V. , Scribano, M. L. , Berto, E. , Luzi, C. , & Andreoli, A. (1993). Development of the Perceived Stress Questionnaire: a new tool for psychosomatic research. Journal of psychosomatic research, 37(1), 19–32. doi:10.1016/0022-3999(93)90120-5
- Licht, C. M. , De Geus, E. J. , Van Dyck, R. , & Penninx, B. W. (2009). Association between anxiety disorders and heart rate variability in The Netherlands Study of Depression and Anxiety (NESDA). Psychosomatic medicine, 71(5), 508–518. doi:10.1097/PSY.0b013e3181a292a6
- Marmot, M. G. , Stansfeld, S. , Patel, C. , North, F. , Head, J. , White, I. &ldots;Smith, G. D. (1991). Health inequalities among British civil servants: the Whitehall II study. The Lancet, 337(8754), 1387–1393. doi:10.1016/0140-6736(91)93068-K
- Masi, C. M. , Hawkley, L. C. , Rickett, E. M. , & Cacioppo, J. T. (2007). Respiratory sinus arrhythmia and diseases of aging: Obesity, diabetes mellitus, and hypertension. Biological psychology, 74(2), 212–223. doi:10.1016/j.biopsycho.2006.07.006
- McClelland, D. C. (2000). Human motivation. CUP Archive.
- Munich Re. (2014). doi:10.1016/j.cmpb.2004.03.004
- Peltola, M. , Tulppo, M. P. , Kiviniemi, A. , Hautala, A. J. , Seppänen, T. , Barthel, P. &ldots;Mäkikallio, T. H. (2008). Respiratory sinus arrhythmia as a predictor of sudden cardiac death after myocardial infarction. Annals of medicine, 40(5), 376–382.
- Penwell, L. , & Larkin, K. (2010). Social support and risk for cardiovascular disease and cancer: A qualitative review examining the role of inflammatory processes. Health Psychology Review, 4, 42–55. doi:10.1080/17437190903427546
- Perakakis, P. , Joffily, M. , Taylor, M. , Guerra, P. , & Vila, J. (2010). KARDIA: A Matlab software for the analysis of cardiac interbeat intervals. Computer methods and programs in biomedicine, 98(1), 83–89. doi:10.1016/j.cmpb.2009.10.002
- Reed, J. , & Buck, S. (2009). The effect of regular aerobic exercise on positive-activated affect: A meta-analysis. Psychology of Sport and Exercise, 10(6), 581–594. doi:10.1016/j.psychsport.2009.05.009
- Reinhard, F. , & Maercker, A. (2004). Sekundäre traumatisierung, posttraumatische belastungsstörung, burnout und soziale unterstützung bei medizinischem rettungspersonal. Zeitschrift für Medizinische Psychologie, 13(1), 29–36.
- Reyes del Paso, G. A. , Garrido, S. , Pulgar, Á. , Mart\'\in-Vázquez, M. , & Duschek, S. (2010). Aberrances in autonomic cardiovascular regulation in fibromyalgia syndrome and their relevance for clinical pain reports. Psychosomatic Medicine, 72(5), 462–470. doi:10.1097/PSY.0b013e3181da91f1
- Reyes del Paso, G. A. , Langewitz, W. , Mulder, L. J. , Roon, A. , & Duschek, S. (2013). The utility of low frequency heart rate variability as an index of sympathetic cardiac tone: a review with emphasis on a reanalysis of previous studies. Psychophysiology, 50(5), 477–487. doi:10.1111/psyp.12027
- Ritchie, E. C. , Watson, P. J. , & Friedman, M. J. (2006). Interventions following mass violence and disasters: Strategies for mental health practice. Guilford Publications.
- Rozanski, A. , & Kubzansky, L. D. (2005). Psychologic functioning and physical health: a paradigm of flexibility. Psychosomatic medicine, 67, S47–S53. doi:10.1097/01.psy.0000164253.69550.49
- Saynaeve, G. (2001). Psycho-social support in situations of mass emergency: A european policy paper concerning different aspects of psychosocial support and social accompaniment for people involved in major accidents and disasters. Brussels: Ministry of Public Health.
- Schnall, P. L. , Landsbergis, P. A. , & Baker, D. (1994). Job strain and cardiovascular disease. Annual review of public health, 15(1), 381–411. doi:10.1146/annurev.pu.15.050194.002121
- Smith, A. M. , Loving, T. J. , Crockett, E. E. , & Campbell, L. (2009). What's closeness got to do with it? Men's and women's cortisol responses when providing and receiving support. Psychosomatic Medicine, 71(8), 843–851. doi:10.1097/PSY.0b013e3181b492e6
- Svensson, E. , Angelborg-Thanderz, M. , & Sjöberg, L. (1993). Mission challenge, mental workload and performance in military aviation. Aviation, space, and environmental medicine.
- Tan, G. , Dao, T. K. , Farmer, L. , Sutherland, R. J. , & Gevirtz, R. (2011). Heart rate variability (HRV) and posttraumatic stress disorder (PTSD): A pilot study. Applied psychophysiology and biofeedback, 36(1), 27–35. doi:10.1007/s10484-010-9141-y
- Taylor, S. E. (2010). Social support: A review. In Friedman, H.S. (Eds.). The Oxford handbook of health psychology.
- Uchino, B. N. , Cacioppo, J. T. , & Kiecolt-Glaser, J. K. (1996). The relationship between social support and physiological processes: a review with emphasis on underlying mechanisms and implications for health. Psychological bulletin, 119(3), 488.
- Van Der Ploeg, E. , & Kleber, R. J. (2003). Acute and chronic job stressors among ambulance personnel: predictors of health symptoms. Occupational and environmental medicine, 60(suppl 1), i40–i46. doi:10.1136/oem.60.suppl_1.i40
- von Zerssen, D. , & Petermann, F. (2011). Beschwerden-Liste - Revidierte Fassung (BL-R). Hogrefe: Göttingen, Germany.
- Zuckerman, M. (1990). The psychophysiology of sensation seeking. Journal of personality, 58(1), 313–345.
Footnotes
1. The following stimuli were selected: crisis-related images 3001, 3010, 3030, 3051, 3059, 3064, 3071, 3101, 3103, 3120, 3130, 3180, 3181, 3185, 3191; general stress images 1525, 1930, 6211, 6231, 6250, 6300, 6315, 6350, 6510, 6520, 6560, 6563, 6570, 6838, 6840; pleasant images 2071, 2080, 2340, 4220, 4520, 4599, 4607, 4608, 4652, 4658, 4659, 4660, 4668, 4676, 4800.
2. Stimuli 277, 319 and 403 were selected.